National Foundations and Infrastructure
National e-health infrastructure is a broad umbrella term for components that are required for many aspects of health information communication. Infrastructure is believed by some to include the standards, architectural approaches, specifications and conformance criteria to enable e-health to be implemented safely and efficiently. More importantly, however, infrastructure is the physical manifestation of components and services built to enable health information communication.
The distinction between the specification of infrastructure components and the actual existence of infrastructure components is probably the most serious deficiency in understanding by the majority of people involved in e-health in Australia. The meaning of ‘e-health infrastructure’ has been hijacked and perverted by a number of people in key roles, such as the CEO and the Chair of NEHTA.
In no other sector of human endeavour has such a perversion of the concept occurred to such an extent. Infrastructure and foundations are concepts from the world of engineering, not from medicine nor banking nor policy making nor management. When we talk of transport infrastructure for the nation, we mean roads, rail lines, shipping ports, signalling systems, traffic lights, etc. Not their mere designs or specifications. When we talk of foundations for a new hospital building, we are referring to the holes in the ground, the steel and concrete, the subfloor plumbing. We do not say the foundations are in place the moment the draftsman finishes her drawings or the moment the electrical contractors hand over their designs and plans.
For e-health, what does this mean? In order to provide the right information to the right person at the right place at the right time, we need key e-health foundations and key infrastructure to actually be in place. We need things built. Standards and specifications do not, of themselves magically build such infrastructure.
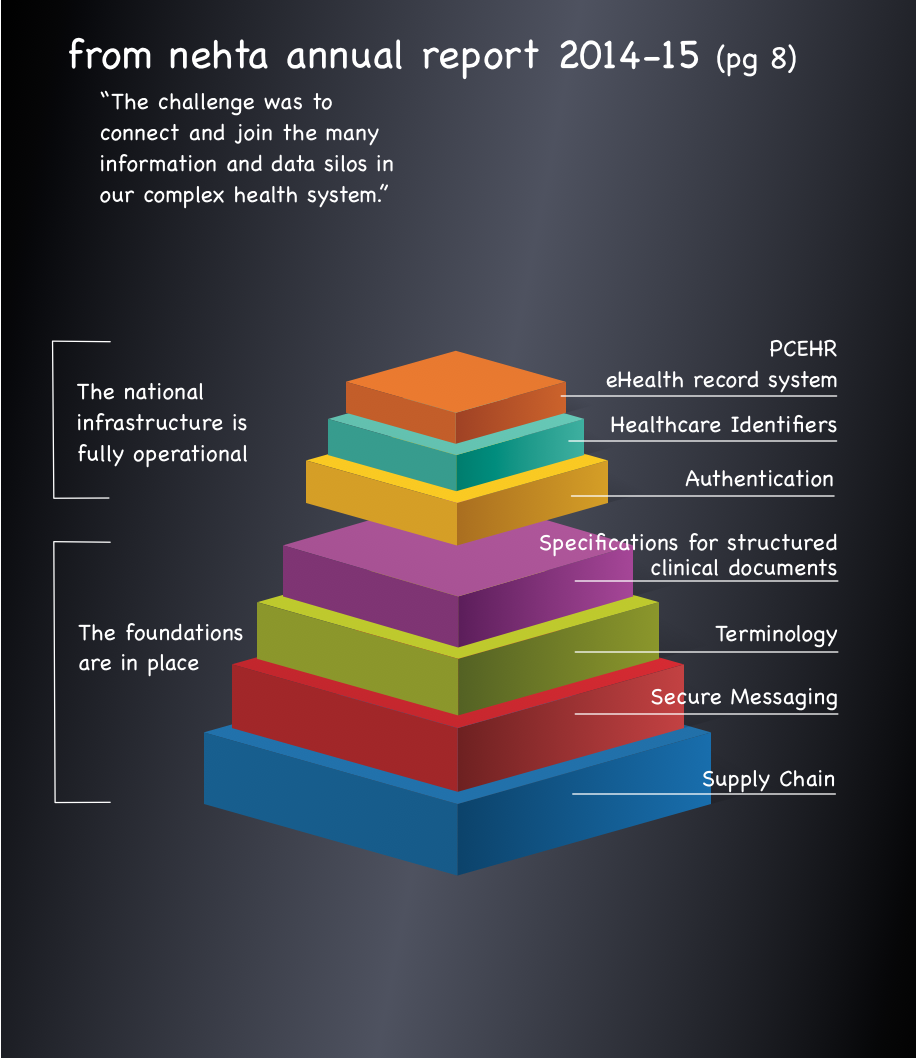
In its 2014-15 annual report and ever since, NEHTA mischievously has tried to pretend that the foundations are in place and that the national infrastructure is fully operational and that the many information and data silos in our complex health system are now joined.
Australia does not have a functioning secure messaging system. It has specifications for parts of such a system. But some critical components are incomplete. Meanwhile, a number of privately run networks comprise the working infrastructure used for day to day communications within their private networks.
Australia does not have the foundation terminology in place to support interoperable data exchange between clinical systems. The few terminology sets that NEHTA produced are not in embedded in any but a small number of clinical systems.
The healthcare identifier services have significant problems and are insufficient to meet the needs of e-health across the nation. Provider identifiers, provider directories and their associated services, particularly linking and location services, are nowhere near adequate for the roles they need to play.
We are also missing the required infrastructure to enable patients to safely and securely communicate directly with their doctors and vice-versa.
Australia does not have a functioning secure messaging system. It has specifications for parts of such a system. But some critical components are incomplete. Meanwhile, a number of privately run networks comprise the working infrastructure used for day to day communications within their private networks.
Australia does not have the foundation terminology in place to support interoperable data exchange between clinical systems. The few terminology sets that NEHTA produced are not in embedded in any but a small number of clinical systems.
The healthcare identifier services have significant problems and are insufficient to meet the needs of e-health across the nation. Provider identifiers, provider directories and their associated services, particularly linking and location services, are nowhere near adequate for the roles they need to play.
We are also missing the required infrastructure to enable patients to safely and securely communicate directly with their doctors and vice-versa.